2017 marked the 15th year of the Safe Motherhood Project in Guatemala. To recap, the Safe Motherhood Project is an educational project to train traditional Mayan Midwifes (Comadronas) in safe birthing techniques and emergency skills in caring for women who have their babies at home. Each course is 5 days long. We now have a competent team of 3 Guatemalan midwives who do the bulk of the teaching. We strive to conduct 3 to 4 courses per year each course attended by 30 Comadronas and/or Paramedics. The Canadian members of the project comprise 2 midwives, 1 family physician, and 1 maternity nurse. We Canadians visit at our own expense
2017 marked the 15th year of the Safe Motherhood Project in Guatemala. To recap, the Safe Motherhood Project is an educational project to train traditional Mayan Midwifes (Comadronas) in safe birthing techniques and emergency skills in caring for women who have their babies at home. Each course is 5 days long. We now have a competent team of 3 Guatemalan midwives who do the bulk of the teaching. We strive to conduct 3 to 4 courses per year each course attended by 30 Comadronas and/or Paramedics. The Canadian members of the project comprise 2 midwives, 1 family physician, and 1 maternity nurse. We Canadians visit at our own expense
once a year in February to make sure the project is on track or to provide practice updates. To date we have taught over 1000 Comadronas in various communities in many parts of the country.
 Since our last report, the team has made 2 visits to Chisec, in the department of Alta Verapaz and has been able to teach 3 courses and a total of 100 comadronas in this municipality. Educational space and meals were generously provided by Karen and Rocky of Compelling Love Ministries, a couple from Kamloops who have acquired a small acreage in Chisec to provide community health education programs and to create a children’s nutritional center. As I write this report, our Guatemalan team will be teaching for 2 weeks, roughly 60 students, in Chichicastenango, a large market community in the highlands of the department of Quiche.
Since our last report, the team has made 2 visits to Chisec, in the department of Alta Verapaz and has been able to teach 3 courses and a total of 100 comadronas in this municipality. Educational space and meals were generously provided by Karen and Rocky of Compelling Love Ministries, a couple from Kamloops who have acquired a small acreage in Chisec to provide community health education programs and to create a children’s nutritional center. As I write this report, our Guatemalan team will be teaching for 2 weeks, roughly 60 students, in Chichicastenango, a large market community in the highlands of the department of Quiche.
Efforts have been made to connect with local Guatemalan NGOs to collaborate materially and financially on this project. Unfortunately, while we receive lots of approval and verbal support, material support at a local level has not been forthcoming. I believe the reality for this project in Guatemala, as with much of the health and education infrastructure in the country, is a dependence on foreign donations for sustainability. A positive development in this country strapped for health dollars is that the Comadronas have been recognized since 2014 as an essential part of the health care system. The government has made efforts to credential Comadronas who receive formal training. We have received official recognition of our course from several levels of government.
 This coming February 2018, the Canadian team members will return to Guatemala for 2 weeks of courses. The community is to be determined. However, the popularity of our course has increased by “word of mouth” and there are several communities requesting our presence. The need is still there for this educational program. We are proud that we have been able to continue this project for 15 years and look forward the project continuing for many more years to come.
This coming February 2018, the Canadian team members will return to Guatemala for 2 weeks of courses. The community is to be determined. However, the popularity of our course has increased by “word of mouth” and there are several communities requesting our presence. The need is still there for this educational program. We are proud that we have been able to continue this project for 15 years and look forward the project continuing for many more years to come.

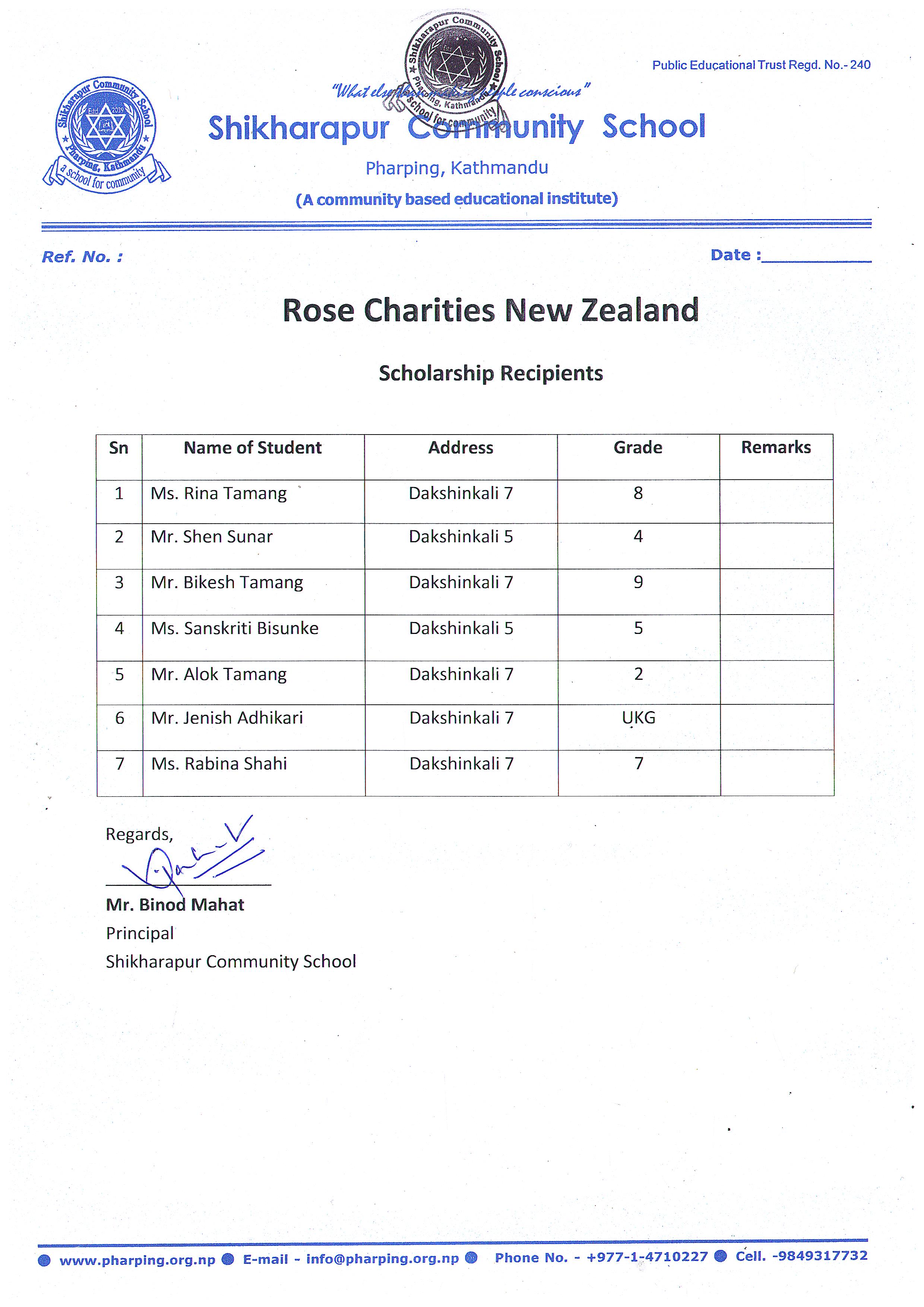
 Rose Charities NZ has worked with Ms Sarala Adhikari (Rose in Nepal) to cooperate with the Shikharapur Community School (Principal Mr Binod Mahat, Campus Chief , Mr Niroj Shrestha) in the beautiful and holy Pharping area in the Kathmandu Valley Nepal. http://www.rigpawiki.org/index.php?title=Pharping
Rose Charities NZ has worked with Ms Sarala Adhikari (Rose in Nepal) to cooperate with the Shikharapur Community School (Principal Mr Binod Mahat, Campus Chief , Mr Niroj Shrestha) in the beautiful and holy Pharping area in the Kathmandu Valley Nepal. http://www.rigpawiki.org/index.php?title=Pharping