The amazing One Tree Hill Sinfonia is holding a charity concert for Malambo Grassroots Zambia Saturday 15th September.
The Malambo Programs are supported through Rose Charities Canada and carry out amazing and hugely needed work in child education, including music education, income generation, womens groups, and health. One of their main organizers is Heidi Krutzen, Canada’s leading harpist currently living and working with the London Philharmonia.
For over 20 years Rose Charities has been developing essential ground level programs to many parts of the world, with no administration fees.
6pm Sat 15th September. Admission 10pounds, St Augustines Church, Honour Oak Park SE23
Rose Charities UK is assisting in provided much needed aid relief to the devastating series of earthquakes which have occurred in Lombok, Indonesia. Working with our Board Member Khalid Virani who was in the region at the time of the quakes, knows the area well and has a reliable network of contacts on the ground we are providing relief supplies such as non perishable food including rice and cooking oil, drinking water, ponchos, tarpaulin and basic medical materials to help alleviate the ongoing
Well over 250 people are confirmed dead, thousands missing or injured and tens of thousands displaced from their homes. Any donations hugely appreciated. Rose Charities UK takes no administration costs and works locally where needs can be met at ground level
Donate through our JustGiving site – please state ‘Lombok’ in the ‘comments/notes’ field
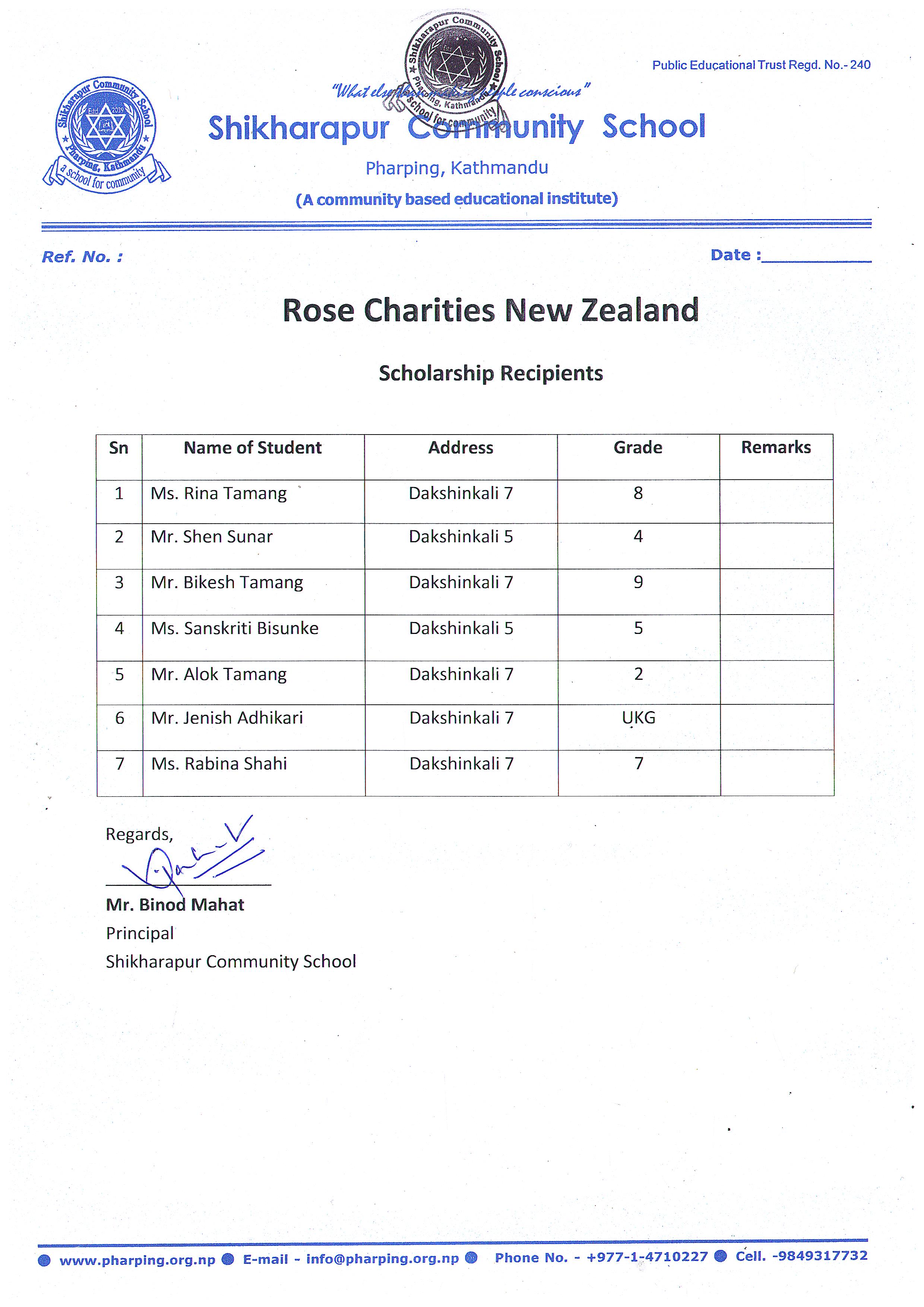
Rose Charities NZ has worked with Ms Sarala Adhikari (Rose in Nepal) to cooperate with the Shikharapur Community School (Principal Mr Binod Mahat, Campus Chief , Mr Niroj Shrestha) in the beautiful and holy Pharping area in the Kathmandu Valley Nepal. http://www.rigpawiki.org/index.php?title=Pharping
Rose Charities NZ provided the funds for an entire and much needed new rood for the school in return for 7 students to be sponsored to grade 10 and 2 to even higher level.
It is anticipated that this program will meet with every success for the girls and will lead on to further cooperative efforts to increase support (especially female) education both in Nepal and worldwide.
Shikharapur Community School has close links with Tribhuvan University Kathmandu.

 The amazing One Tree Hill Sinfonia is holding a charity concert for Malambo Grassroots Zambia Saturday 15th September.
The amazing One Tree Hill Sinfonia is holding a charity concert for Malambo Grassroots Zambia Saturday 15th September.